
📖 Step 2 — Learning Material
This topic uses the AIM Learning Cycle to help MBBS students understand the structural organization of the peritoneum and its spaces by integrating Anatomy and Clinical concepts.
🔹 1️⃣ Introduction
The peritoneum is the largest serous membrane of the body and plays a crucial role in supporting abdominal organs and allowing their smooth movement during digestion. It is located within the abdominal and pelvic cavities, lining the walls and covering the viscera. The peritoneum forms folds, sacs, ligaments, and recesses that organize the abdominal organs and provide pathways for blood vessels and nerves.
Clinically, understanding the peritoneum is essential because infections, fluid collections, internal hernias, and abdominal surgeries involve these spaces. Conditions such as peritonitis, ascites, and internal hernias directly relate to peritoneal anatomy.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Peritoneum → A continuous serous membrane lining the abdominal cavity and covering abdominal organs.
- Parietal peritoneum → Lines abdominal wall.
- Visceral peritoneum → Covers abdominal organs.
- Peritoneal cavity → Potential space between parietal and visceral layers containing small amount of fluid.
- Mesentery → Double layer of peritoneum attaching organs to posterior abdominal wall.
- Omentum → Peritoneal fold connecting stomach to other organs.
- Peritoneal ligament → Double-layered peritoneal fold connecting organ to organ or wall.
- Sac → Large peritoneal compartment (greater sac or lesser sac).
- Recess → Small pocket formed by peritoneal folds.
- Pouch → Dependent space where fluid accumulates.
🔹 3️⃣ Core Learning — Curriculum Coverage
1. GREATER OMENTUM
CORE
• A large apron-like fold of peritoneum hanging from the greater curvature of stomach.
• Located anterior to intestines, covering abdominal organs.
• Extends downward from stomach, then folds upward to attach to transverse colon.
• Made of four layers of peritoneum.
• Contains:
o Fat deposits
o Blood vessels
o Lymphatics
o Immune cells
• Major Blood Supply:
o Right gastroepiploic artery (from gastroduodenal artery)
o Left gastroepiploic artery (from splenic artery)
• Function:
o Protection
o Fat storage
o Infection control
o Insulation
CONCEPT EXPLAINED
The greater omentum develops from the dorsal mesogastrium. It hangs like an apron in front of the intestines, forming a protective barrier. Because it contains fat and immune cells, it can move toward inflamed areas, such as an infected appendix.
Structure → Function Logic:
• Large surface area → Covers intestines
• Fat content → Cushions organs
• Mobility → Helps isolate infection
It acts like the “policeman of the abdomen”, limiting spread of infection.
 IF DAMAGED
IF DAMAGED
Cause: Injury or infection
Effect:
• Reduced infection containment
• Spread of peritonitis
• Increased risk of abscess formation
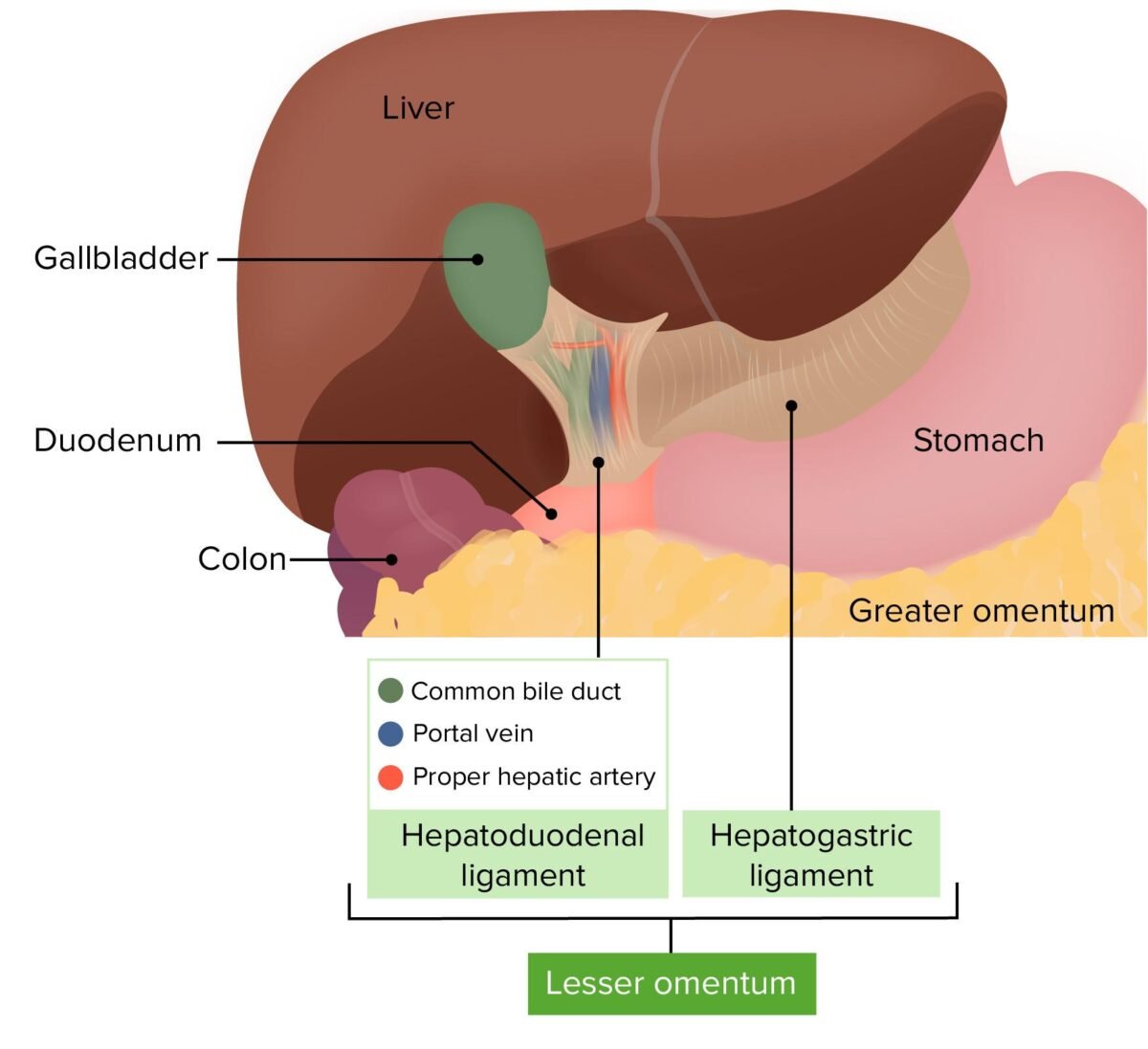
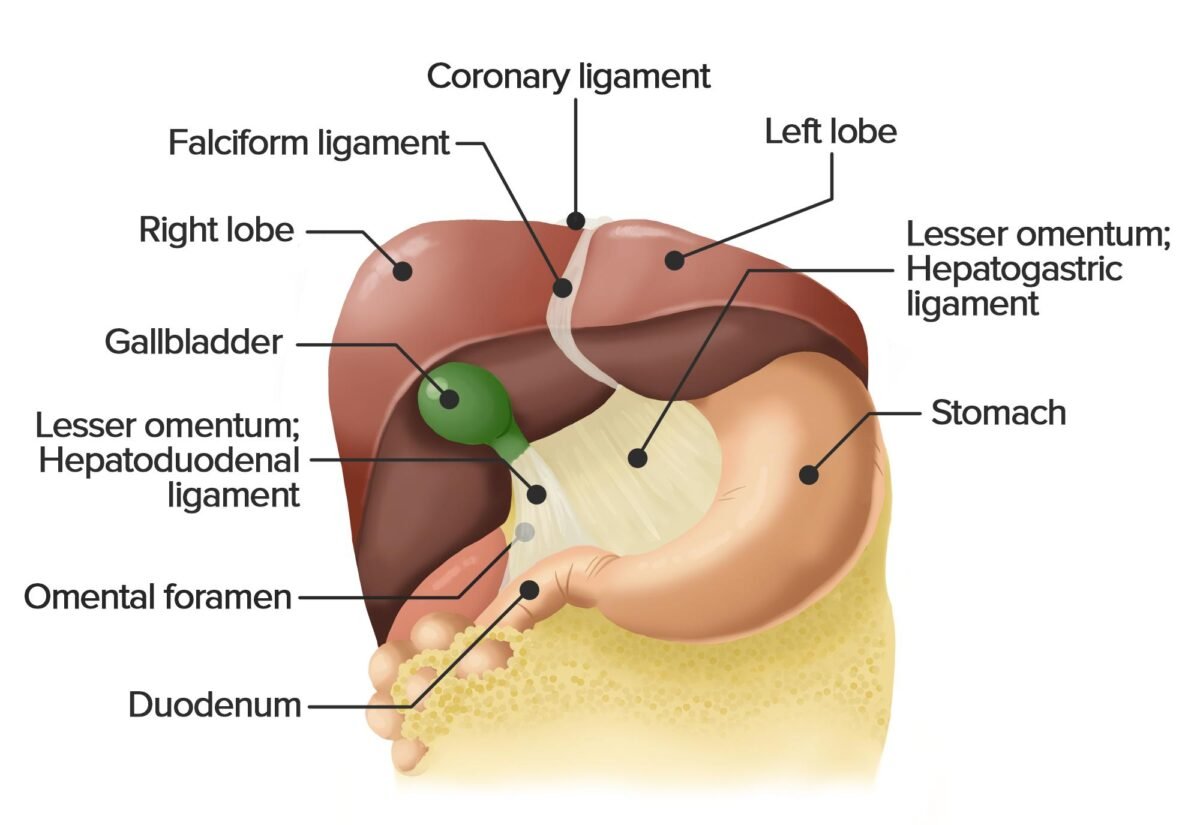
2. LESSER OMENTUM
CORE
• Thin double-layered peritoneal fold.
• Connects:
o Liver → Lesser curvature of stomach
o Liver → First part of duodenum
• Located between liver and stomach.
• Parts:
o Hepatogastric ligament
o Hepatoduodenal ligament
• Contents of hepatoduodenal ligament:
o Portal vein
o Hepatic artery proper
o Common bile duct
• Blood Supply:
o Hepatic arterial branches
Primary Function:
• Provides pathway for major vessels entering liver.
CONCEPT EXPLAINED
The lesser omentum develops from the ventral mesogastrium. It acts as a support structure holding the liver in position while allowing passage of vessels.
Structure → Function Logic:
Thin membrane → Flexible movement
Strong attachments → Stable vascular pathway
IF DAMAGED
Cause: Trauma or surgery
Effect:
• Portal triad injury
• Severe bleeding
• Bile leakage
3. NERVE SUPPLY OF PERITONEUM
CORE
Two types of innervation:
Parietal Peritoneum
• Somatic nerve supply
• Highly sensitive to:
o Pain
o Pressure
o Temperature
Nerves:
• Lower intercostal nerves
• Lumbar nerves
• Phrenic nerve (central diaphragm)
Visceral Peritoneum
• Autonomic nerve supply
• Sensitive to:
o Stretch
o Chemical irritation
Nerves:
• Sympathetic nerves
• Parasympathetic nerves
 CONCEPT EXPLAINED
CONCEPT EXPLAINED
Parietal peritoneum has somatic nerves similar to skin, so pain is sharp and localized.
Visceral peritoneum has autonomic nerves, so pain is dull and poorly localized.
Structure → Function Logic:
Somatic nerves → Precise localization
Autonomic nerves → Diffuse visceral pain
IF DAMAGED
Cause: Inflammation (peritonitis)
Effect:
• Sharp localized pain when parietal peritoneum involved
• Guarding of abdominal wall
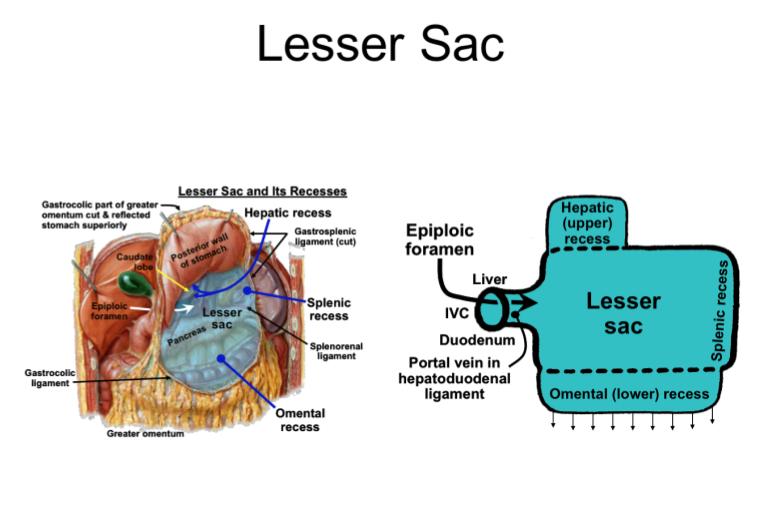
4. LESSER SAC (OMENTAL BURSA)
CORE
• A peritoneal cavity space located posterior to stomach.
• Lies between stomach and pancreas.
• Communicates with greater sac through epiploic foramen.
• Boundaries:
Anterior:
• Stomach
• Lesser omentum
Posterior:
• Pancreas
Superior:
• Liver
Inferior:
• Transverse colon
Function:
• Allows free movement of stomach.
CONCEPT EXPLAINED
The lesser sac forms due to rotation of the stomach during development. It creates a space behind the stomach, allowing stomach expansion during digestion.
Structure → Function Logic:
Posterior cavity → Allows stomach mobility
IF DAMAGED
Cause: Pancreatitis
Effect:
• Fluid accumulation in lesser sac
• Abscess formation
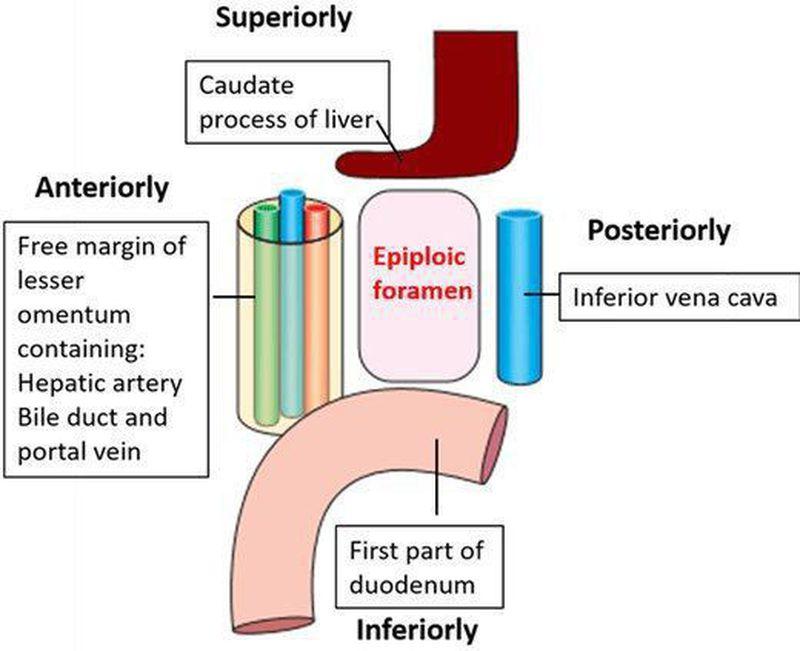
5. BOUNDARIES OF EPIPLOIC FORAMEN
CORE
Also called Foramen of Winslow.
Connects:
• Lesser sac ↔ Greater sac
Boundaries:
Anterior:
• Hepatoduodenal ligament
Posterior:
• Inferior vena cava
Superior:
• Caudate lobe of liver
Inferior:
• First part of duodenum
Contents:
• Passage between sacs
CONCEPT EXPLAINED
The epiploic foramen acts as a gateway between peritoneal compartments.
Structure → Function Logic:
Small opening → Controls communication between sacs
IF DAMAGED
Cause: Internal hernia
Effect:
• Intestinal obstruction
• Compromised blood supply
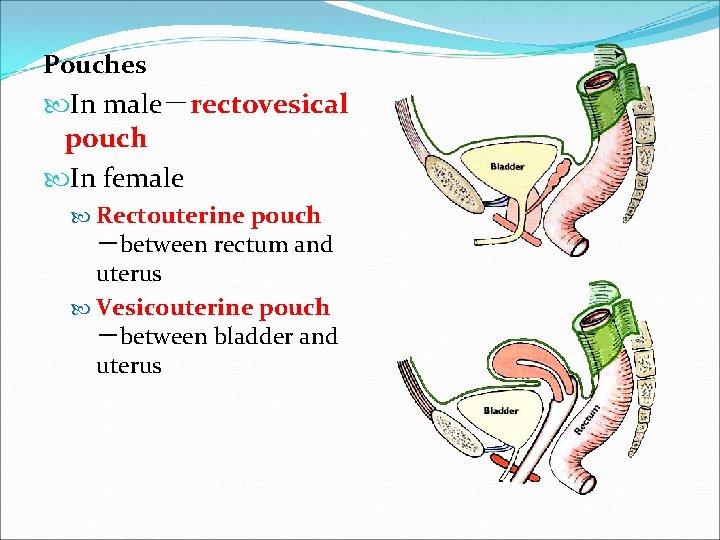
6. PERITONEAL POUCHES
CORE
Spaces where fluid accumulates.
Male
• Rectovesical pouch
o Between rectum and bladder
Female
• Uterovesical pouch
• Rectouterine pouch (Pouch of Douglas)
Function:
• Lowest point of peritoneal cavity
• Fluid collection site
CONCEPT EXPLAINED
Gravity causes fluid (blood, pus, ascites) to collect in dependent regions.
Structure → Function Logic:
Dependent location → Fluid accumulation
IF DAMAGED
Cause: Infection
Effect:
• Abscess formation
• Pelvic pain
7. PERITONEAL RECESSES
CORE
Small pockets formed by folds of peritoneum.
Examples:
• Duodenal recess
• Cecal recess
• Intersigmoid recess
Function:
• Allows organ movement
CONCEPT EXPLAINED
These recesses are spaces formed during gut rotation.
Structure → Function Logic:
Folds → Space formation → Organ flexibility
IF DAMAGED
Cause: Herniation
Effect:
• Internal hernia
• Intestinal obstruction
8. PERITONEAL LIGAMENTS
CORE
Double-layered folds connecting organs.
Examples:
• Falciform ligament
• Gastrosplenic ligament
• Splenorenal ligament
Function:
• Organ stabilization
• Vessel support
CONCEPT EXPLAINED
Ligaments act as structural supports carrying vessels.
Structure → Function Logic:
Double layer → Strength + vessel passage
IF DAMAGED
Cause: Trauma
Effect:
• Organ displacement
• Bleeding
9. Retroperitoneal Organs and Clinical Spread of Infection in Peritoneal Spaces
Retroperitoneal Organs
Some abdominal organs are not completely covered by peritoneum. These organs lie behind the peritoneal cavity and are called retroperitoneal organs.
Primary retroperitoneal organs develop behind the peritoneum from the beginning.
Examples:
-
Kidneys
-
Ureters
-
Suprarenal glands
-
Abdominal aorta
-
Inferior vena cava
Secondary retroperitoneal organs were initially intraperitoneal during development but later became fixed to the posterior abdominal wall.
Examples:
-
Duodenum, except first part
-
Pancreas, except tail
-
Ascending colon
-
Descending colon
-
Upper two-thirds of rectum
Clinical Importance
Retroperitoneal organs are clinically important because infection, hemorrhage, or malignancy involving these organs may spread behind the peritoneal cavity and may not initially produce obvious peritoneal signs.
Examples:
-
Pancreatitis may spread inflammation into retroperitoneal tissue.
-
Renal infection may spread in the retroperitoneal space.
-
Retroperitoneal bleeding may remain hidden initially.
Subhepatic Space, Morison’s Pouch, and Spread of Infection
The subhepatic space lies inferior to the liver. Its most clinically important part is the hepatorenal recess, also called Morison’s pouch.
Morison’s pouch is located between:
-
Right lobe of liver anteriorly/superiorly
-
Right kidney and suprarenal gland posteriorly/inferiorly
Connection with the Right Paracolic Gutter
The right subhepatic space communicates freely with the right paracolic gutter. Because of this communication, fluid, blood, pus, or infected material from the upper abdomen may spread downward along the right paracolic gutter.
This is clinically important in:
-
Appendicitis
-
Perforated duodenal ulcer
-
Liver abscess rupture
-
Gallbladder infection
-
Peritonitis
Infection may collect in the right subhepatic space or Morison’s pouch, especially in the supine position.
Right and Left Paracolic Gutters
The paracolic gutters are vertical peritoneal channels located lateral to the ascending and descending colon.
Right Paracolic Gutter
The right paracolic gutter is clinically more important because it provides a free communication between the pelvis and the right subhepatic space.
Therefore, infected fluid from the pelvis or right lower abdomen may ascend to the right subhepatic space.
Example:
In acute appendicitis, pus may travel upward through the right paracolic gutter and collect in the right subhepatic space.
Left Paracolic Gutter
The left paracolic gutter is less freely continuous with the upper abdomen because the phrenicocolic ligament acts as a partial barrier.
Therefore, infection from the left lower abdomen is more likely to remain localized or spread toward the pelvis rather than freely reaching the left subphrenic or left subhepatic region.
Dependent Peritoneal Spaces in Different Positions
The site where fluid collects depends on body position.
In Supine Position
When the patient is lying on the back, the most dependent spaces are:
-
Hepatorenal recess / Morison’s pouch
-
Pelvic cavity
-
Paracolic gutters
Morison’s pouch is especially important in supine patients because free intraperitoneal fluid commonly collects there.
In Erect Position
When the patient is standing or sitting upright, fluid tends to move downward under the effect of gravity and collects mainly in:
-
Rectovesical pouch in males
-
Rectouterine pouch of Douglas in females
These are the most dependent parts of the peritoneal cavity in the erect position.
Clinical Correlation
Free fluid, blood, pus, bile, or gastric contents may spread through peritoneal recesses and gutters. Therefore, understanding the communication between the subhepatic space, Morison’s pouch, and paracolic gutters helps explain the clinical spread of abdominal infection.
For example:
-
In perforated duodenal ulcer, fluid may collect in the right subhepatic space.
-
In appendicitis, infection may spread upward through the right paracolic gutter.
-
In females, pelvic fluid may collect in the rectouterine pouch.
-
In males, pelvic fluid may collect in the rectovesical pouch.
⚙️ 4️⃣ Functional Flow
Peritoneal Structure → Space Formation → Fluid Movement → Protection → Clinical Outcome
Peritoneum develops into greater and lesser sacs, forming omentum and peritoneal ligaments that connect abdominal organs.
↓
Greater and lesser omentum suspend organs and carry vessels, lymphatics, and nerves.
↓
Peritoneal pouches and recesses create dependent spaces where fluids collect according to gravity.
↓
Lesser sac communicates with greater sac through the epiploic foramen, allowing movement of fluid within the peritoneal cavity.
↓
Nerve supply of peritoneum determines pain localization (parietal → sharp, visceral → dull).
↓
Functional Outcome:
Protection of abdominal organs, distribution of fluids, localization of infection, and compartmentalization of pathological processes.
🩺 5️⃣ Clinical Correlation
1️⃣ Peritonitis
Cause: Infection or perforation of abdominal organ (e.g., appendix, ulcer).
Effect:
- Severe localized pain (parietal peritoneum involvement)
- Guarding and rigidity
- Fluid accumulation in peritoneal pouches
Clinical Link:
Dependent spaces like rectovesical pouch or pouch of Douglas collect infected fluid.
2️⃣ Ascites
Cause: Liver disease, portal hypertension, malignancy.
Effect:
- Fluid accumulates in greater sac and peritoneal pouches
- Abdominal distension
- Shifting dullness on examination
Clinical Link:
Fluid collects in most dependent peritoneal recesses.
3️⃣ Internal Herniation Through Epiploic Foramen
Cause: Bowel loop entering lesser sac through epiploic foramen.
Effect:
- Intestinal obstruction
- Severe abdominal pain
Clinical Link:
Knowledge of boundaries of epiploic foramen is critical in surgery.
4️⃣ Spread of Infection Through Lesser Sac
Cause: Posterior gastric perforation or pancreatitis.
Effect:
- Infection spreads into lesser sac
- Retroperitoneal inflammation
Clinical Link:
Lesser sac acts as a potential infection compartment.
5️⃣ Referred Pain in Peritoneal Irritation
Cause: Irritation of visceral peritoneum.
Effect:
- Dull poorly localized pain
- Later becomes sharp when parietal peritoneum involved
Clinical Link:
Different nerve supply explains pain characteristics.
📌 6️⃣ Summary Points
- Greater omentum hangs from greater curvature of stomach and covers intestines.
- Lesser omentum connects stomach to liver.
- Lesser sac lies posterior to stomach.
- Epiploic foramen connects greater sac and lesser sac.
- Boundaries of epiploic foramen are clinically important in surgery.
- Peritoneal pouches collect fluid according to gravity.
- Peritoneal recesses are potential sites of internal herniation.
- Peritoneal ligaments support abdominal organs and carry vessels.
- Parietal peritoneum pain is sharp and localized.
- Visceral peritoneum pain is dull and poorly localized.
- Ascitic fluid accumulates in dependent peritoneal spaces.
- Peritoneal anatomy is essential for abdominal surgery and diagnosis.