
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Lipoprotein metabolism is the process by which lipids are transported through blood to different tissues of the body. Since fats are insoluble in water, they require special transport particles called lipoproteins. These lipoproteins circulate in plasma and deliver triglycerides and cholesterol to tissues for energy production, membrane synthesis, and hormone formation.
The liver and intestine are the major organs involved in lipoprotein synthesis and metabolism. Proper lipid transport is essential for maintaining energy balance and cellular function. Disorders of lipoprotein metabolism lead to abnormal blood lipid levels known as hyperlipidemia or dyslipidemia.
Clinically, lipid disorders are strongly associated with atherosclerosis, coronary artery disease, stroke, pancreatitis, and metabolic syndrome. Understanding lipoprotein metabolism helps explain why elevated LDL cholesterol is harmful and why HDL cholesterol is protective.
This topic integrates biochemistry with medicine by linking molecular lipid transport mechanisms to common cardiovascular diseases.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Lipoproteins: Complexes of lipids and proteins that transport lipids in blood.
- Apolipoproteins: Protein components of lipoproteins that stabilize structure and act as enzyme activators or receptor ligands.
- Triglycerides (TG): Major storage form of fat used for energy.
- Cholesterol: Structural lipid used in cell membranes, steroid hormones, and bile acids.
- Hyperlipidemia: Increased plasma lipids or lipoproteins.
- Dyslipidemia: Abnormal lipid profile including increased or decreased lipids.
- Atherosclerosis: Deposition of lipid plaques within arterial walls.
- LDL cholesterol: “Bad cholesterol” associated with plaque formation.
- HDL cholesterol: “Good cholesterol” involved in reverse cholesterol transport.
Essential Terminology
- Exogenous pathway: Transport of dietary lipids from intestine.
- Endogenous pathway: Transport of liver-synthesized lipids.
- Reverse cholesterol transport: HDL-mediated movement of cholesterol from tissues back to liver.
- Lipoprotein lipase (LPL): Enzyme that hydrolyzes triglycerides.
- LCAT: Enzyme involved in HDL maturation.
- Foam cells: Lipid-filled macrophages in atherosclerosis.
Basic Overview
- Lipids cannot travel freely in plasma because they are hydrophobic.
- Lipoproteins package lipids into transportable particles.
- Different lipoproteins carry different lipid components.
- Apolipoproteins determine the function and destination of lipoproteins.
- Disturbance in lipid transport causes lipid disorders and vascular disease.
🔹 3️⃣ Core Learning — Curriculum Coverage
Lipoprotein Metabolism and Lipid Disorders
🧠 CORE
- Lipoproteins are lipid-protein complexes that transport triglycerides and cholesterol in blood.
- Major lipoprotein classes are chylomicrons, VLDL, LDL, and HDL.
- Lipoproteins contain triglycerides, cholesterol, phospholipids, and apolipoproteins.
- Apolipoproteins stabilize lipoproteins and regulate enzyme activation and receptor binding.
- Chylomicrons transport dietary triglycerides from intestine to tissues.
- VLDL transports endogenous triglycerides synthesized in liver.
- LDL delivers cholesterol to peripheral tissues.
- HDL removes excess cholesterol from tissues and returns it to liver.
- Lipoprotein metabolism maintains lipid transport, energy balance, and cholesterol homeostasis.
- Disturbances in lipid metabolism cause hyperlipidemia and dyslipidemia.
🔬 CONCEPT EXPLAINED
Lipids are hydrophobic molecules and cannot circulate freely in plasma. The body solves this problem by packaging lipids into lipoproteins. Each lipoprotein has a hydrophobic lipid core surrounded by phospholipids and apolipoproteins that make the particle water soluble.
Structure of Lipoproteins
Lipoproteins consist of:
- Core: Triglycerides and cholesterol esters
- Surface: Phospholipids, free cholesterol, and apolipoproteins
The amount of lipid and protein determines density:
- More triglyceride → lower density
- More protein → higher density
Thus:
- Chylomicrons are least dense
- HDL is most dense
Classes of Lipoproteins
1. Chylomicrons
- Largest lipoproteins
- Formed in intestinal mucosal cells
- Rich in dietary triglycerides
- Contain Apo B-48
- Deliver dietary fat to adipose tissue and muscle
2. VLDL (Very Low Density Lipoprotein)
- Produced by liver
- Carry endogenous triglycerides
- Contain Apo B-100
- Deliver liver-synthesized lipids to tissues
3. LDL (Low Density Lipoprotein)
- Derived from VLDL metabolism
- Cholesterol-rich particle
- Delivers cholesterol to peripheral tissues
- Major atherogenic lipoprotein
4. HDL (High Density Lipoprotein)
- Synthesized in liver and intestine
- Rich in Apo A-I
- Performs reverse cholesterol transport
- Protective against atherosclerosis
Functions of Apolipoproteins
Apolipoproteins determine the metabolic behavior of lipoproteins.
Important Apolipoproteins
| Apolipoprotein | Major Function |
|---|---|
| Apo A-I | Activates LCAT |
| Apo B-48 | Chylomicron formation |
| Apo B-100 | LDL receptor binding |
| Apo C-II | Activates lipoprotein lipase |
| Apo E | Hepatic uptake of remnants |
These proteins:
- Stabilize lipoproteins
- Activate enzymes
- Help receptor recognition
- Regulate lipid transport
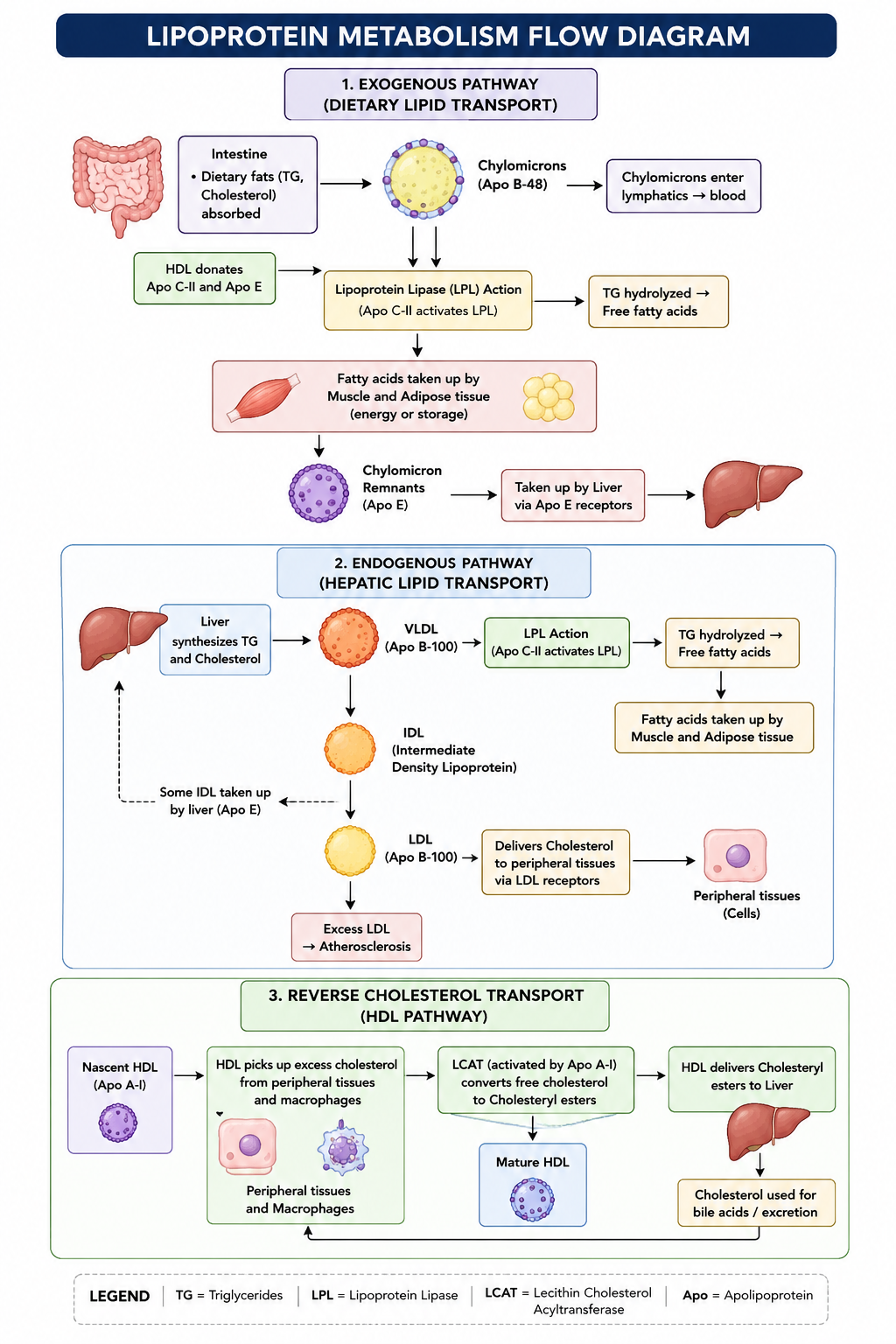
Chylomicron Metabolism
After fat absorption:
- Dietary triglycerides are absorbed in intestine.
- Intestinal cells form chylomicrons.
- Chylomicrons enter lymphatics then blood.
- HDL transfers Apo C-II and Apo E to chylomicrons.
- Apo C-II activates lipoprotein lipase (LPL).
- LPL breaks triglycerides into fatty acids.
- Fatty acids enter muscle and adipose tissue.
- Chylomicron remnants are taken up by liver via Apo E receptors.
Why This Pathway Exists
It transports dietary fat efficiently from intestine to tissues for:
- Energy production
- Fat storage
- Cellular functions
VLDL Metabolism
The liver synthesizes triglycerides from excess carbohydrates and fatty acids.
Process
- Liver packages triglycerides into VLDL.
- VLDL enters circulation.
- LPL removes triglycerides.
- VLDL becomes IDL.
- IDL is converted into LDL.
Functonal Importance
This pathway distributes endogenous lipids produced by liver.
LDL Metabolism
LDL is the major cholesterol transport particle.
Functions
- Delivers cholesterol to cells
- Supports membrane synthesis
- Required for steroid hormone production
Mechanism
- LDL binds LDL receptors via Apo B-100.
- Cells internalize LDL by receptor-mediated endocytosis.
- Cholesterol is released inside cells.
Clinical Importance
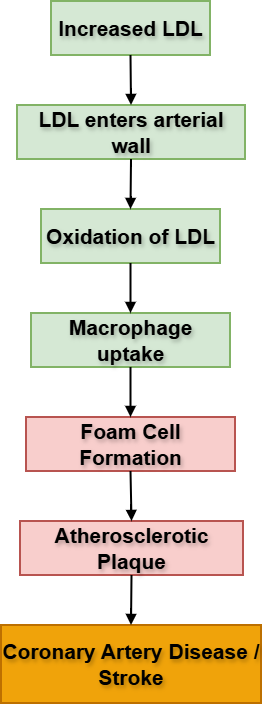
Excess LDL enters arterial walls where macrophages engulf oxidized LDL forming foam cells and atherosclerotic plaques.
HDL Metabolism
HDL performs reverse cholesterol transport.
Mechanism
- HDL collects excess cholesterol from tissues.
- Apo A-I activates LCAT.
- Cholesterol becomes esterified.
- HDL transports cholesterol back to liver.
- Liver excretes cholesterol through bile.
Why HDL is Protective
HDL prevents cholesterol accumulation in blood vessels and reduces atherosclerosis risk.
Lipid Disorders
Hyperlipidemia and Dyslipidemia
Hyperlipidemia
Increased plasma levels of:
- Cholesterol
- Triglycerides
- Lipoproteins
Dyslipidemia
Abnormal lipid profile including:
- High LDL
- High triglycerides
- Low HDL
Classification of Hyperlipidemia
| Type | Main Lipoprotein Increased |
|---|---|
| Type I | Chylomicrons |
| Type IIa | LDL |
| Type IIb | LDL + VLDL |
| Type III | IDL remnants |
| Type IV | VLDL |
| Type V | VLDL + Chylomicrons |
Enzyme Deficiencies
Lipoprotein Lipase Deficiency
- Triglycerides cannot be hydrolyzed
- Severe hypertriglyceridemia develops
- Increased pancreatitis risk
LDL Receptor Deficiency
- LDL clearance decreases
- Familial hypercholesterolemia occurs
- Premature coronary artery disease develops
LCAT Deficiency
- HDL maturation impaired
- Reverse cholesterol transport reduced
Epidemiology of Hyperlipidemia
Risk factors include:
- Obesity
- Sedentary lifestyle
- Diabetes mellitus
- High-fat diet
- Smoking
- Family history
- Aging
Modern lifestyle changes have greatly increased the prevalence of dyslipidemia worldwide.
Preventive Strategies
Lifestyle Measures
- Healthy balanced diet
- Reduced saturated fat intake
- Regular exercise
- Weight reduction
- Smoking cessation
Medical Prevention
- Lipid screening
- Statin therapy
- Diabetes control
- Blood pressure control
Diseases Associated with Hyperlipidemia
Atherosclerosis
- Lipid deposition in arterial walls
- Plaque formation
- Reduced blood flow
Coronary Artery Disease
- Narrowing of coronary arteries
- Angina and myocardial infarction
Stroke
- Cerebral vessel obstruction
Acute Pancreatitis
- Severe hypertriglyceridemia may inflame pancreas
Fatty Liver Disease
- Excess triglyceride accumulation in liver
⚠️ IF DAMAGED
Defects in lipoprotein metabolism cause abnormal lipid accumulation in blood and tissues.
Cause → Effect Relationships
- LPL deficiency → severe hypertriglyceridemia → pancreatitis
- LDL receptor defect → elevated LDL → atherosclerosis
- Low HDL → impaired cholesterol removal → cardiovascular disease
- Excess VLDL production → fatty liver and dyslipidemia
- Oxidized LDL deposition → foam cell formation → plaque development
Failure of lipid homeostasis ultimately increases the risk of:
- Coronary artery disease
- Stroke
- Peripheral vascular disease
- Sudden cardiac death
VLDL, LDL, and HDL Metabolism
🧠 CORE
VLDL (Very Low Density Lipoprotein)
- Produced in liver
- Rich in endogenous triglycerides
- Contains Apo B-100
- Delivers triglycerides to tissues
- Lipoprotein lipase (LPL) removes triglycerides
- VLDL converts into IDL then LDL
LDL (Low Density Lipoprotein)
- Derived from VLDL metabolism
- Rich in cholesterol
- Contains Apo B-100
- Delivers cholesterol to peripheral tissues
- Binds LDL receptors
- Major atherogenic lipoprotein
HDL (High Density Lipoprotein)
- Synthesized in liver and intestine
- Rich in Apo A-I
- Performs reverse cholesterol transport
- Activates LCAT
- Removes excess cholesterol from tissues
- Protective against atherosclerosis
🔬 CONCEPT EXPLAINED
The liver synthesizes triglycerides from excess carbohydrates and fatty acids. These triglycerides are packaged into VLDL particles and released into blood circulation.
VLDL Metabolism
In circulation:
- VLDL receives Apo C-II from HDL.
- Apo C-II activates lipoprotein lipase (LPL).
- LPL hydrolyzes triglycerides into fatty acids.
- Fatty acids enter muscle and adipose tissue.
- As triglycerides decrease, VLDL becomes smaller and denser.
- VLDL converts into IDL.
- Further triglyceride removal converts IDL into LDL.
This pathway distributes liver-produced lipids to body tissues.
LDL Metabolism
LDL is the major cholesterol transport particle in blood.
Cells require cholesterol for:
- Cell membrane formation
- Steroid hormone synthesis
- Vitamin D synthesis
- Bile acid formation
LDL binds LDL receptors through Apo B-100 and enters cells by receptor-mediated endocytosis.
When LDL levels become excessive:
- LDL enters arterial walls
- LDL undergoes oxidation
- Macrophages engulf oxidized LDL
- Foam cells form
- Atherosclerotic plaques develop
Thus LDL is strongly associated with cardiovascular disease.
HDL Metabolism
HDL performs reverse cholesterol transport, which protects blood vessels from cholesterol accumulation.
Mechanism
- HDL collects excess cholesterol from peripheral tissues and macrophages.
- Apo A-I activates LCAT.
- LCAT converts free cholesterol into cholesterol esters.
- Cholesterol esters become trapped within HDL.
- HDL transports cholesterol back to liver.
In the liver, cholesterol may be:
- Reused
- Converted into bile acids
- Excreted in bile
Thus HDL acts as a protective lipoprotein against atherosclerosis.
⚠️ IF DAMAGED
Excess VLDL Production
Causes:
- Hypertriglyceridemia
- Fatty liver
- Increased cardiovascular risk
Commonly associated with:
- Diabetes mellitus
- Obesity
- Alcohol excess
Elevated LDL Levels
Cause:
- Atherosclerotic plaque formation
- Coronary artery disease
- Stroke
- Peripheral vascular disease
Familial hypercholesterolemia occurs due to LDL receptor defects.
Low HDL Levels
Result in:
- Reduced reverse cholesterol transport
- Increased cholesterol deposition in vessels
- Increased atherosclerosis risk
- Higher incidence of coronary artery disease
- Metabolic syndrome complications
Epidemiology, Prevention, and Diseases Associated with Hyperlipidemia
🧠 CORE
Epidemiology of Hyperlipidemia
Risk increases with:
- Obesity
- Sedentary lifestyle
- Diabetes mellitus
- High-fat diet
- Smoking
- Increasing age
- Family history
Hyperlipidemia is one of the major global risk factors for cardiovascular disease.
Preventive Strategies
Prevention includes:
- Healthy balanced diet
- Regular exercise
- Weight control
- Smoking cessation
- Lipid profile screening
- Control of diabetes and hypertension
- Statin therapy when indicated
Diseases Associated with Hyperlipidemia
Major associated diseases:
- Atherosclerosis
- Coronary artery disease
- Stroke
- Peripheral vascular disease
- Acute pancreatitis
- Fatty liver disease
🔬 CONCEPT EXPLAINED
Modern lifestyle changes have significantly increased the prevalence of lipid disorders worldwide.
Epidemiological Factors
Urbanization, reduced physical activity, and excessive intake of calorie-rich foods promote obesity and insulin resistance, leading to dyslipidemia.
Diabetes mellitus commonly causes:
- Increased triglycerides
- Increased VLDL
- Reduced HDL
Genetic predisposition also contributes to familial hyperlipidemia.
As age increases, lipid metabolism becomes less efficient, increasing cardiovascular risk.
Preventive Strategies and Their Functional Importance
Lifestyle modification improves lipid metabolism and reduces cardiovascular complications.
Dietary Measures
- Reduced saturated fat intake lowers LDL cholesterol.
- Increased fiber intake improves cholesterol excretion.
Exercise
Regular physical activity:
- Increases HDL
- Reduces triglycerides
- Improves insulin sensitivity
Weight Reduction
Decreases:
- VLDL production
- Triglyceride levels
- Cardiovascular risk
Smoking Cessation
Smoking damages vascular endothelium and lowers HDL levels. Stopping smoking improves vascular protection.
Statin Therapy
Statins inhibit hepatic cholesterol synthesis by inhibiting HMG-CoA reductase, resulting in:
- Reduced LDL levels
- Reduced atherosclerosis progression
- Lower cardiovascular mortality
Diseases Associated with Hyperlipidemia
Atherosclerosis
Excess LDL accumulates in arterial walls causing:
- Foam cell formation
- Plaque development
- Arterial narrowing
Coronary Artery Disease
Plaque formation in coronary arteries reduces myocardial blood supply and may cause:
- Angina
- Myocardial infarction
Stroke
Atherosclerosis in cerebral vessels may obstruct blood flow leading to ischemic stroke.
Peripheral Vascular Disease
Reduced blood flow to limbs causes:
- Claudication
- Tissue ischemia
Acute Pancreatitis
Severe hypertriglyceridemia can trigger pancreatic inflammation.
Fatty Liver Disease
Excess triglyceride accumulation in hepatocytes leads to nonalcoholic fatty liver disease (NAFLD).
⚠️ IF DAMAGED
Failure of lipid control and preventive measures leads to progressive vascular injury and organ damage.
Cause → Effect Relationships
- Obesity + sedentary lifestyle → dyslipidemia → atherosclerosis
- Increased LDL → arterial plaque formation → coronary artery disease
- Severe hypertriglyceridemia → pancreatic inflammation → pancreatitis
- Fat accumulation in liver → fatty liver disease
- Progressive plaque formation → myocardial infarction and stroke
Advanced Complications
- Organ ischemia
- Heart failure
- Sudden cardiac death
- Premature mortality
⚙️ 4️⃣ Functional Flow
Chylomicron Metabolism
- Dietary fats absorbed in intestine
- Chylomicrons formed with Apo B-48
- Enter lymphatics → blood
- Gain Apo C-II and Apo E from HDL
- LPL hydrolyzes triglycerides
- Fatty acids enter tissues
- Chylomicron remnants return to liver
VLDL → LDL Pathway
- Liver synthesizes triglycerides
- VLDL released into blood
- LPL removes triglycerides
- VLDL becomes IDL
- IDL becomes LDL
- LDL delivers cholesterol to tissues
HDL Reverse Cholesterol Transport
- HDL collects cholesterol from tissues
- Apo A-I activates LCAT
- Cholesterol esterified
- HDL carries cholesterol to liver
- Liver excretes cholesterol in bile
🩺 5️⃣ Clinical Correlation
Familial Hypercholesterolemia
- LDL receptor defect
- Very high LDL levels
- Premature coronary artery disease
Type I Hyperlipoproteinemia
- LPL deficiency
- Massive hypertriglyceridemia
- Pancreatitis
Atherosclerosis
- LDL accumulation in arterial walls
- Foam cell formation
- Plaque development
Metabolic Syndrome
Associated with:
- Obesity
- Diabetes
- Hypertension
- Dyslipidemia
Xanthomas
- Lipid deposits in skin/tendons
- Seen in severe hyperlipidemia
📌 6️⃣ Summary Points
- Lipoproteins transport insoluble lipids in blood.
- Chylomicrons carry dietary triglycerides.
- VLDL transports endogenous triglycerides from liver.
- LDL is the major cholesterol carrier.
- HDL performs reverse cholesterol transport.
- Apo C-II activates lipoprotein lipase.
- Apo B-100 binds LDL receptors.
- Elevated LDL promotes atherosclerosis.
- Low HDL increases cardiovascular risk.
- Familial hypercholesterolemia is caused by LDL receptor defects.
- Severe hypertriglyceridemia can cause pancreatitis.
- Lifestyle modification is the cornerstone of prevention.