
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
The large intestine forms the terminal part of the gastrointestinal tract and is responsible for absorption of water, formation of feces, and temporary storage of waste before defecation. It begins at the cecum in the right iliac fossa and extends to the anal canal in the perineum. Structurally, the large intestine differs from the small intestine by the presence of taeniae coli, haustra, and appendices epiploicae.
The rectum and anal canal are specialized terminal segments that regulate continence and defecation. The anal canal is clinically important because structures above and below the pectinate line differ in blood supply, nerve supply, lymphatic drainage, and pain sensation.
Understanding this topic is essential for recognizing common conditions such as appendicitis, hemorrhoids, anal fissure, rectal prolapse, and ischiorectal abscess. Knowledge of spatial anatomy also helps in clinical examination and interpretation of radiological images.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Large intestine: Terminal part of gut extending from ileocecal junction to anus.
- Cecum: Blind pouch located below ileocecal junction.
- Colon: Main tubular part of large intestine.
- Rectum: Distal straight segment storing feces before defecation.
- Anal canal: Terminal passage between rectum and anus.
- Mesocolon: Double layer of peritoneum attaching parts of colon to posterior abdominal wall.
- Pectinate line: Important landmark dividing upper and lower anal canal.
Essential Terminology
- Taeniae coli: Three longitudinal muscle bands of colon.
- Haustra: Sacculations produced by tone of taeniae coli.
- Appendices epiploicae: Fat-filled peritoneal tags on colon.
- Ischiorectal fossa: Fat-filled wedge-shaped space beside anal canal.
- Internal hemorrhoids: Dilated veins above pectinate line.
- External hemorrhoids: Dilated veins below pectinate line.
Basic Overview
The large intestine consists of:
- Cecum
- Ascending colon
- Transverse colon
- Descending colon
- Sigmoid colon
- Rectum
- Anal canal
Major functions:
- Absorption of water and electrolytes
- Formation and storage of feces
- Defecation
- Maintenance of continence
🔹 3️⃣ Core Learning — Curriculum Coverage
Section 1 — Large Intestine: Gross Anatomy
Cecum
🧠 CORE
- Blind pouch of large intestine.
- Located in right iliac fossa.
- Lies below ileocecal junction.
- Continuous superiorly with ascending colon.
- Vermiform appendix arises from posteromedial wall.
- Intraperitoneal structure.
- Supplied by ileocolic artery.
- Main function: initiation of water absorption and mixing of intestinal contents.
🔬 CONCEPT EXPLAINED
The cecum is the first part of the large intestine and acts as a receiving chamber for contents entering from the ileum. It lies in the right lower abdomen and is usually completely covered by peritoneum, making it mobile.
Three taeniae coli converge at the base of the appendix, an important surgical landmark. The wide lumen allows temporary collection of intestinal contents before propulsion into ascending colon.
Structure → Function
- Wide blind pouch → slows intestinal flow.
- Large diameter → permits mixing and bacterial action.
- Relation with appendix → clinically important in appendicitis.
⚠️ IF DAMAGED
- Obstruction → cecal distension.
- Inflammation of appendix → right iliac fossa pain.
- Loss of motility → fecal stasis and infection.
Ascending Colon
🧠 CORE
- Extends from cecum to hepatic flexure.
- Located on right side of abdomen.
- Retroperitoneal structure.
- Contains taeniae coli and haustra.
- Posterior relations include quadratus lumborum and right kidney.
- Supplied mainly by right colic artery.
- Absorbs water and electrolytes.
- Moves fecal material upward.
🔬 CONCEPT EXPLAINED
The ascending colon carries fecal contents upward toward the transverse colon. Being retroperitoneal provides stability and prevents excessive mobility.
The longitudinal muscle bands shorten the colon wall, producing sacculations called haustra. These increase surface area and facilitate slow movement for water absorption.
Structure → Function
- Fixed retroperitoneal position → stability.
- Haustra → slow transit for absorption.
- Large lumen → accommodates semisolid feces.
⚠️ IF DAMAGED
- Obstruction → abdominal distension.
- Reduced absorption → diarrhea.
- Tumors → bowel obstruction and anemia.
Transverse Colon
🧠 CORE
- Longest and most mobile part of colon.
- Extends between hepatic and splenic flexures.
- Intraperitoneal structure.
- Attached by transverse mesocolon.
- Crosses abdomen horizontally.
- Supplied by middle colic artery.
- Participates in water absorption.
- Stores and transports fecal matter.
🔬 CONCEPT EXPLAINED
The transverse colon hangs freely due to its mesentery, allowing movement during digestion. The splenic flexure is higher and more fixed than hepatic flexure.
The transverse mesocolon carries blood vessels, lymphatics, and nerves to the colon. Mobility allows accommodation of abdominal organ movement.
Structure → Function
- Mesocolon → mobility with vascular support.
- Wide lumen → fecal transport.
- Haustra → delayed transit for absorption.
⚠️ IF DAMAGED
- Volvulus may occur in mobile colon.
- Ischemia at splenic flexure due to weak blood supply.
- Inflammation → abdominal pain and altered bowel habits.
Descending Colon
🧠 CORE
- Extends from splenic flexure to sigmoid colon.
- Located on left side of abdomen.
- Retroperitoneal structure.
- Narrower lumen than ascending colon.
- Supplied by left colic artery.
- Stores semisolid feces.
- Posteriorly related to left kidney and abdominal wall muscles.
🔬 CONCEPT EXPLAINED
The descending colon functions mainly in storage and further dehydration of feces. Retroperitoneal fixation stabilizes the bowel.
Its narrower diameter reflects progression toward more solid fecal content.
Structure → Function
- Fixed position → efficient downward movement.
- Narrow lumen → compaction of feces.
- Muscular wall → propulsion toward sigmoid colon.
⚠️ IF DAMAGED
- Obstruction causes constipation.
- Diverticular disease commonly affects left colon.
- Reduced motility → fecal accumulation.
Sigmoid Colon
🧠 CORE
- S-shaped terminal part of colon.
- Located in left iliac fossa and pelvis.
- Intraperitoneal.
- Attached by sigmoid mesocolon.
- Highly mobile segment.
- Supplied by sigmoid arteries.
- Stores feces before rectum.
- Common site of volvulus.
🔬 CONCEPT EXPLAINED
The sigmoid colon acts as a temporary storage chamber for feces before defecation. Its mesentery gives considerable mobility.
The curved shape allows expansion during fecal accumulation. Excessive mobility, however, predisposes to twisting.
Structure → Function
- Mobility → expansion and storage.
- Muscular wall → fecal propulsion.
- Curved shape → accommodates increasing fecal mass.
⚠️ IF DAMAGED
- Volvulus → intestinal obstruction.
- Ischemia → bowel necrosis.
- Chronic constipation → excessive dilation.
Mesentery of Large Intestine
🧠 CORE
- Double layer of peritoneum.
- Supports mobile parts of colon.
- Includes transverse mesocolon and sigmoid mesocolon.
- Contains blood vessels, lymphatics, and nerves.
- Provides mobility while maintaining vascular connection.
- Prevents twisting of bowel.
- Allows passage of neurovascular structures.
🔬 CONCEPT EXPLAINED
Mesocolon suspends the intestine from posterior abdominal wall while carrying essential vessels and nerves.
The transverse and sigmoid colon require mobility for filling and movement of feces, therefore mesentery permits movement without interrupting blood supply.
Structure → Function
- Double peritoneal layers → flexible support.
- Neurovascular contents → nourishment and control.
- Mobility → prevents tension during bowel filling.
⚠️ IF DAMAGED
- Vascular compromise → ischemia.
- Mesenteric twisting → volvulus.
- Infection spread through lymphatics.
![]()
Section 2 — Rectum & Anal Canal
Gross Anatomy of Rectum
🧠 CORE
- Terminal straight part of large intestine.
- Extends from sigmoid colon to anal canal.
- Located within pelvis.
- Follows sacral curvature.
- Has transverse rectal folds.
- Upper third covered by peritoneum anteriorly and laterally.
- Stores feces before defecation.
- Supplied by superior rectal artery.
🔬 CONCEPT EXPLAINED
The rectum acts as a reservoir for feces. Its dilatable wall allows temporary storage before defecation reflex occurs.
Three lateral rectal folds help support fecal matter and prevent sudden passage into anal canal. The rectum follows curvature of sacrum, helping maintain continence.
Structure → Function
- Distensible wall → storage.
- Curved course → controlled defecation.
- Strong muscular wall → expulsion during defecation.
⚠️ IF DAMAGED
- Loss of rectal tone → incontinence.
- Rectal prolapse → protrusion through anus.
- Tumors → bleeding and obstruction.
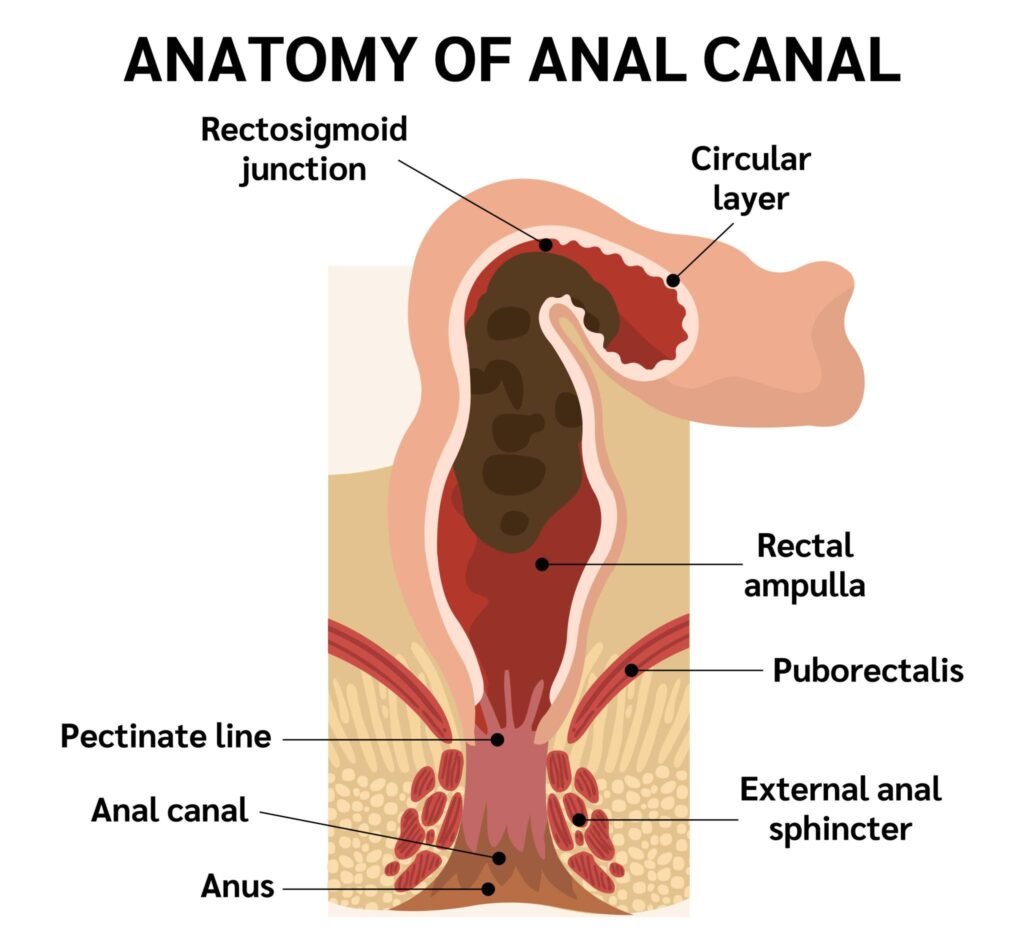
Gross Anatomy of Anal Canal
🧠 CORE
- Terminal 3–4 cm of gastrointestinal tract.
- Extends from rectum to anus.
- Divided by pectinate line.
- Contains anal columns and anal valves.
- Surrounded by internal and external sphincters.
- Upper part supplied by autonomic nerves.
- Lower part supplied by somatic nerves.
- Maintains continence.
🔬 CONCEPT EXPLAINED
The anal canal regulates passage of feces and continence. The pectinate line marks embryological transition between endodermal and ectodermal parts.
The internal sphincter is smooth muscle and involuntary, while external sphincter is skeletal muscle and voluntary. Together they maintain continence.
Muscle Rule
Internal Anal Sphincter
- Origin: Circular smooth muscle of rectum
- Insertion: Surrounds upper anal canal
- Action: Involuntary constriction
- Functional role: Maintains resting continence
External Anal Sphincter
- Origin: Perineal structures around anal canal
- Insertion: Encircles anal canal
- Action: Voluntary constriction
- Functional role: Conscious control of defecation
Nerve Supply Logic
- Pudendal nerve → external sphincter → voluntary continence → injury causes fecal incontinence.
⚠️ IF DAMAGED
- Sphincter injury → fecal incontinence.
- Damage below pectinate line → severe pain.
- Infection → fistula formation.
Section 3 — Blood Supply & Clinical Correlation
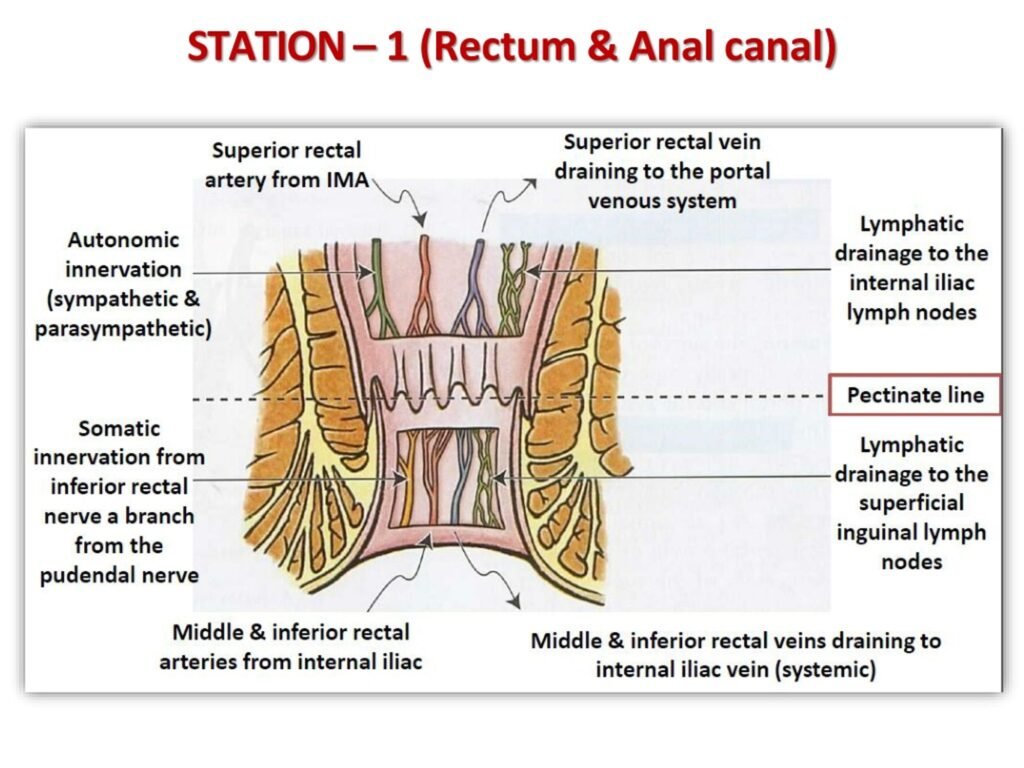
Blood Supply of Anal Canal
🧠 CORE
- Upper anal canal supplied by superior rectal artery.
- Superior rectal artery arises from inferior mesenteric artery.
- Lower anal canal supplied by inferior rectal artery.
- Inferior rectal artery arises from internal pudendal artery.
- Venous plexuses surround anal canal.
- Portosystemic anastomosis present.
- Different lymphatic drainage above and below pectinate line.
🔬 CONCEPT EXPLAINED
The pectinate line divides two embryological regions with different vascular and nerve supply.
Above pectinate line:
- Visceral innervation
- Less pain sensitive
- Portal venous drainage
Below pectinate line:
- Somatic innervation
- Highly pain sensitive
- Systemic venous drainage
Structure → Function
- Rich vascular plexus → cushions anal canal during continence.
- Dual venous drainage → communication between portal and systemic systems.
⚠️ IF DAMAGED
- Venous dilation → hemorrhoids.
- Portal hypertension → enlarged rectal veins.
- Arterial compromise → ischemic pain.
Clinical Correlates of Anal Canal Blood Supply
🧠 CORE
- Internal hemorrhoids occur above pectinate line.
- External hemorrhoids occur below pectinate line.
- Internal hemorrhoids are usually painless.
- External hemorrhoids are painful.
- Anal fissure commonly occurs in lower canal.
- Portal hypertension enlarges rectal venous plexus.
- Pectinate line is clinically important landmark.
🔬 CONCEPT EXPLAINED
Internal hemorrhoids arise from superior rectal veins and are covered by mucosa with visceral innervation, therefore pain is minimal.
External hemorrhoids arise from inferior rectal veins below pectinate line where somatic sensory nerves produce severe pain.
Structure → Function
- Venous plexus supports closure of canal.
- Increased pressure → venous dilation and hemorrhoids.
⚠️ IF DAMAGED
- Thrombosed veins → severe pain.
- Fissure → painful defecation.
- Chronic bleeding → anemia.
![]()
Section 4 — Ischiorectal (Anal) Fossa
Boundaries of Ischiorectal Fossa
🧠 CORE
- Fat-filled wedge-shaped space beside anal canal.
- Located in anal triangle.
- Lateral boundary: obturator internus muscle.
- Medial boundary: external anal sphincter and levator ani.
- Roof: levator ani.
- Floor: skin and fascia.
- Allows expansion of anal canal during defecation.
🔬 CONCEPT EXPLAINED
The ischiorectal fossa contains fat that permits expansion of anal canal during passage of feces.
The wedge-shaped arrangement allows neurovascular structures to pass through the region safely.
Structure → Function
- Fat-filled space → cushioning and expansion.
- Open communication → spread of infection possible.
⚠️ IF DAMAGED
- Infection → ischiorectal abscess.
- Abscess spread → fistula formation.
- Compression of nerves → pain during sitting.
Contents of Ischiorectal Fossa
🧠 CORE
- Ischioanal fat pad.
- Inferior rectal nerves.
- Inferior rectal vessels.
- Pudendal canal laterally.
- Lymphatics present.
- Supports anal canal function.
- Permits distension during defecation.
🔬 CONCEPT EXPLAINED
The fat pad reduces friction during movement of pelvic floor and anal canal. Inferior rectal vessels and nerves pass through this region to supply anal canal.
Nerve Supply Logic
Inferior rectal nerve → external anal sphincter → voluntary continence → nerve injury causes incontinence.
Structure → Function
- Fat → flexibility and cushioning.
- Neurovascular bundles → maintain anal canal function.
⚠️ IF DAMAGED
- Nerve injury → continence problems.
- Vessel injury → bleeding.
- Infection → abscess formation.
![]()
⚙️ 4️⃣ Functional Flow
| Structure | Function | Outcome |
|---|---|---|
| Taeniae coli | Produce haustra | Slow fecal movement |
| Haustra | Segment fecal material | Water absorption |
| Sigmoid colon | Temporary storage | Controlled defecation |
| Rectum | Fecal reservoir | Defecation reflex |
| Internal sphincter | Involuntary closure | Resting continence |
| External sphincter | Voluntary closure | Conscious continence |
| Ischiorectal fat | Expansion support | Smooth defecation |
🩺 5️⃣ Clinical Correlation
Common Clinical Conditions
- Appendicitis
- Colonic obstruction
- Sigmoid volvulus
- Ulcerative colitis
- Internal hemorrhoids
- External hemorrhoids
- Anal fissure
- Rectal prolapse
- Ischiorectal abscess
- Fistula in ano
📌 6️⃣ Summary Points
- Large intestine is identified by taeniae coli, haustra, and appendices epiploicae.
- Cecum lies in right iliac fossa below ileocecal junction.
- Transverse and sigmoid colon are intraperitoneal.
- Ascending and descending colon are retroperitoneal.
- Pectinate line is major anatomical and clinical landmark.
- Internal hemorrhoids are painless because of visceral innervation.
- External hemorrhoids are painful because of somatic innervation.
- Rectum acts as temporary fecal reservoir.
- Internal anal sphincter is involuntary smooth muscle.
- External anal sphincter is voluntary skeletal muscle.
- Ischiorectal fossa contains fat and inferior rectal neurovascular structures.
- Sigmoid colon is common site for volvulus due to mobility.
Recommended Kenhub Videos
1️⃣ Large Intestine Anatomy
Covers:
Cecum, ascending colon, transverse colon, descending colon, sigmoid colon,
taeniae coli, haustra, and mesocolon.
2️⃣ Rectum & Anal Canal Anatomy
Covers:
Rectum, anal canal, pectinate line, sphincters, blood supply,
hemorrhoids, and clinical anatomy.